In the first part of this blog series on child sexual grooming, we focused on uncovering and dispelling myths surrounding grooming, highlighting the ways families are often targeted as part of the grooming process. The second part shifted focus to examine both the short- and long-term effects of child sexual grooming and the intervention strategies available to professionals in their work with victims and their families.
The third part of this series addresses two questions professionals frequently encounter about sexual grooming:
- How can we equip children and parents with the knowledge and skills needed to reduce their risk of victimization?
- What strategies help mental health providers work more effectively with colleagues and community members on this issue?
Knowledge and Skills to Recognize and Avoid Online Grooming
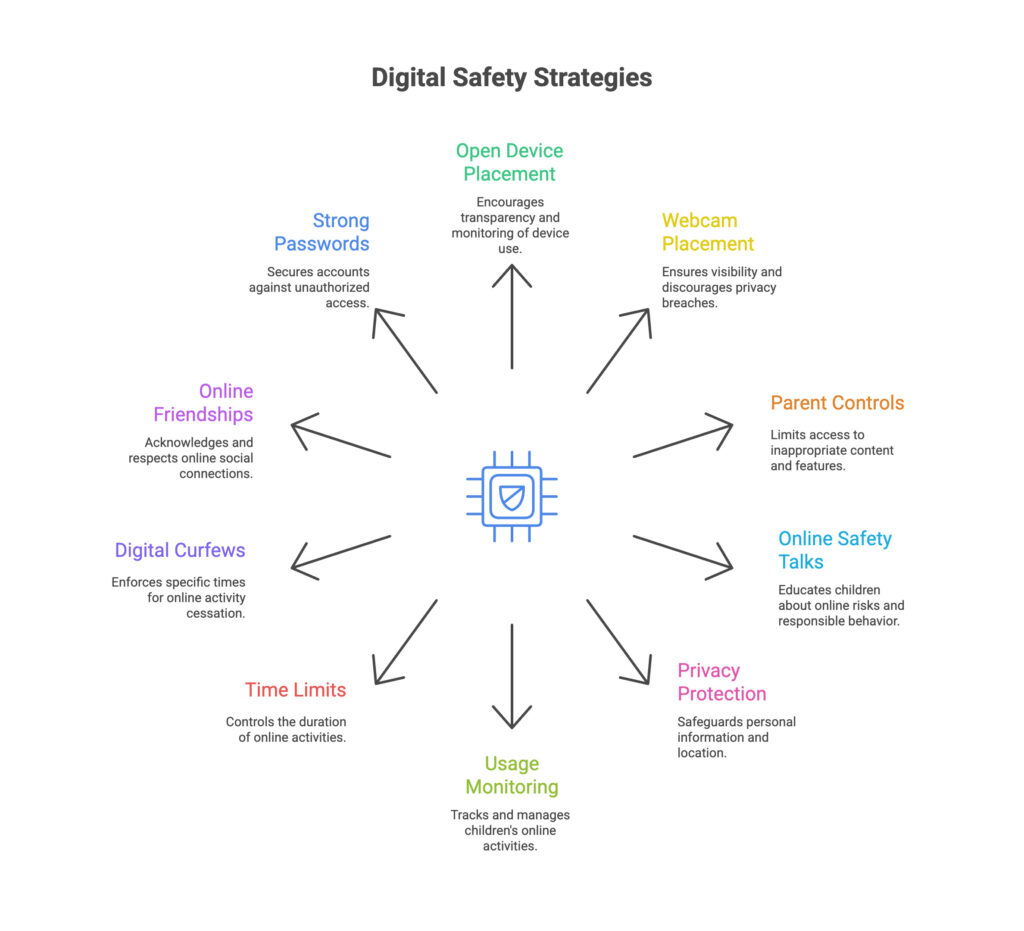
While grooming is most often perpetrated by people known to and trusted by the victims, such as family and extended family members, friends, neighbors, coaches, doctors, pastors, etc., online methods of grooming are increasing in frequency. Today’s online spaces reward quick clicks and constant connection. Individuals who commit harm may try to take advantage of this tendency, especially among young people, to send them to websites and engage them in conversations to start or continue the grooming process. As a result, schools attempt to teach “digital literacy skills” either through direct instruction in how to evaluate the credibility of websites or through class activities such as projects in which students must communicate with each other online. The knowledge gained from these approaches can reduce vulnerability to online grooming by promoting reflection, critical thinking, and healthy boundaries.
Online Safety That Matches Real Life
Despite these activities, school-issued devices and parental control apps are not foolproof—devices can be hacked, and students themselves can find ways to bypass safeguards, sometimes with little effort. There are several additional strategies that parents and therapists can use to enhance online safety for children, including keeping devices in shared spaces, reviewing apps and message histories, and incorporating online friends into everyday conversations. The goal in all these approaches is partnership and visibility, not surveillance alone.
For many caregivers of children under 18, there is a belief that a school-issued tablet will provide protection from nefarious online contact and activities. However, these safeguards are not only limited and penetrable, but they contribute to a false sense of security for caregivers, contributing to children’s unsupervised online activity. Pruitt and Wolf, Child Sexual Grooming: Untangling Myth from Reality to Prevent the Harm of Child Sexual Abuse
Multidisciplinary Teams: What They Are and Why They Help
For victims of grooming and sexual assault, individual therapy, of course, remains essential, but research increasingly shows that a collaborative, multidisciplinary approach produces excellent outcomes for survivors and their families. This coordinated care model, long established in child advocacy centers for investigation purposes, is now expanding into post-disclosure treatment with promising results.
Multidisciplinary teams (MDTs) bring together professionals from different disciplines to work toward a shared goal. In sexual grooming and abuse cases, these teams typically include law enforcement, victim therapists, school counselors, medical providers, and other specialists. Rather than operating in isolation, team members coordinate their efforts, share information, and develop unified treatment approaches.

The collaboration addresses a fundamental challenge in this field: sexual grooming affects multiple domains of a child’s life simultaneously. A victim may need medical care, mental health treatment, educational support, and family intervention all at once. When these services operate independently, gaps emerge, and conflicting approaches can actually impede healing.
Research by Herbert and Bromfelt found that when MDTs were employed:
- The criminal justice system produced more arrests and prosecutions
- Child protection services saw an improvement in response
- An increase in joint investigations and police involvement, and improved quality of collaboration
- The likelihood of medical services increased
- Mental health services were used more often by child survivors, and with improved coordination between providers, child and caregiver satisfaction with the response to the abuse improved
The Information-Sharing Advantage
One of the most powerful aspects of MDTs is their ability to share information that reveals the full scope of grooming behaviors. When team members compare their observations and client reports, they often uncover grooming tactics that weren’t visible to any single provider working alone.
For example, a child’s therapist might learn about a specific grooming strategy used by the individual who caused the harm, such as having the child sit on his lap to watch TV. This information can be shared (with appropriate consents) with the non-offending caregiver’s therapist, who can then help that parent understand how they might have been manipulated and how to better support their child’s healing. Meanwhile, a school counselor on the team can implement classroom strategies that address the child’s specific trauma responses.
This comprehensive understanding helps child survivors feel less shame, confusion, and self-blame while holding individuals more accountable for the full scope of their manipulative behaviors.
Implementation Considerations for Organizations
Organizations considering MDT approaches should start by identifying key stakeholders and potential team members in their community. Child Advocacy Centers offer logical coordination points given their existing relationships with multiple systems and their mandated experience facilitating investigation-focused teams.
The most successful teams begin with clear vision statements and logic models that outline how each stakeholder contributes resources and expertise toward shared outcomes. These foundational planning steps help prevent later conflicts and ensure all team members understand their roles.
Moving Forward: From Isolation to Collaboration
The complexity of sexual grooming’s impact demands responses that match that complexity. While individual therapy will always play a central role in treatment, the evidence increasingly points toward collaborative, multidisciplinary approaches as the most effective way to support healing and prevent future harm.
For mental health professionals, this shift requires moving beyond the traditional model of isolated practice toward one that embraces coordination, information sharing, and shared responsibility for client outcomes. The research suggests that both clients and professionals benefit when this collaborative approach becomes the standard of care rather than the exception.
Read the rest of the posts in this series:
- Part 1: https://safersociety.org/understanding-child-sexual-grooming-part-1-beyond-the-myths-to-the-reality/
- Part 2: https://safersociety.org/understanding-child-sexual-grooming-part-2-short-long-term-effects-on-the-child/
Resources for Professionals
Safer Society’s Continuing Education Center offers several relevant trainings/webinars for professionals interested in developing or improving their collaborative approaches:
- Understanding and Preventing Child Sexual Grooming
- Best Practices in Treatment Planning for Adolescents Who Have Sexually Abused
- Building Prevention Teams to Prevent Child Sexual Abuse
The National Children’s Alliance provides resources for developing and maintaining multidisciplinary teams, and many state-level child advocacy organizations offer training and consultation on team development.